Michigan Dch 3877 PDF Form
The Michigan Department of Community Health has issued an essential bulletin outlining significant revisions to the preadmission screening and annual resident review process, specifically impacting the DCH-3877 and DCH-3878 forms. These updates, effective immediately upon receipt, are of particular interest to nursing facilities, hospitals, and community mental health services programs involved in Medicaid services. The changes are aimed at enhancing the accuracy and efficiency of identifying individuals who require mental health services, with a special focus on those with mental illnesses or developmental disabilities. The transition from the MSA-3877 and MSA-3878 forms to the revised DCH versions includes several critical updates: the shift from the DSM III-R to DSM IV for diagnostic criteria, renaming entities to reflect current organizational structures, and clarifying the criteria for dementia diagnoses and exemptions. Furthermore, the forms offer clear guidance on when and how to complete the screening process, ensuring that those in need of special care are correctly identified and assisted. Providers are encouraged to order or download the updated forms promptly to stay compliant with the state's Medicaid program requirements, and direct any inquiries to the Department of Community Health to ensure smooth implementation of these changes.
Preview - Michigan Dch 3877 Form
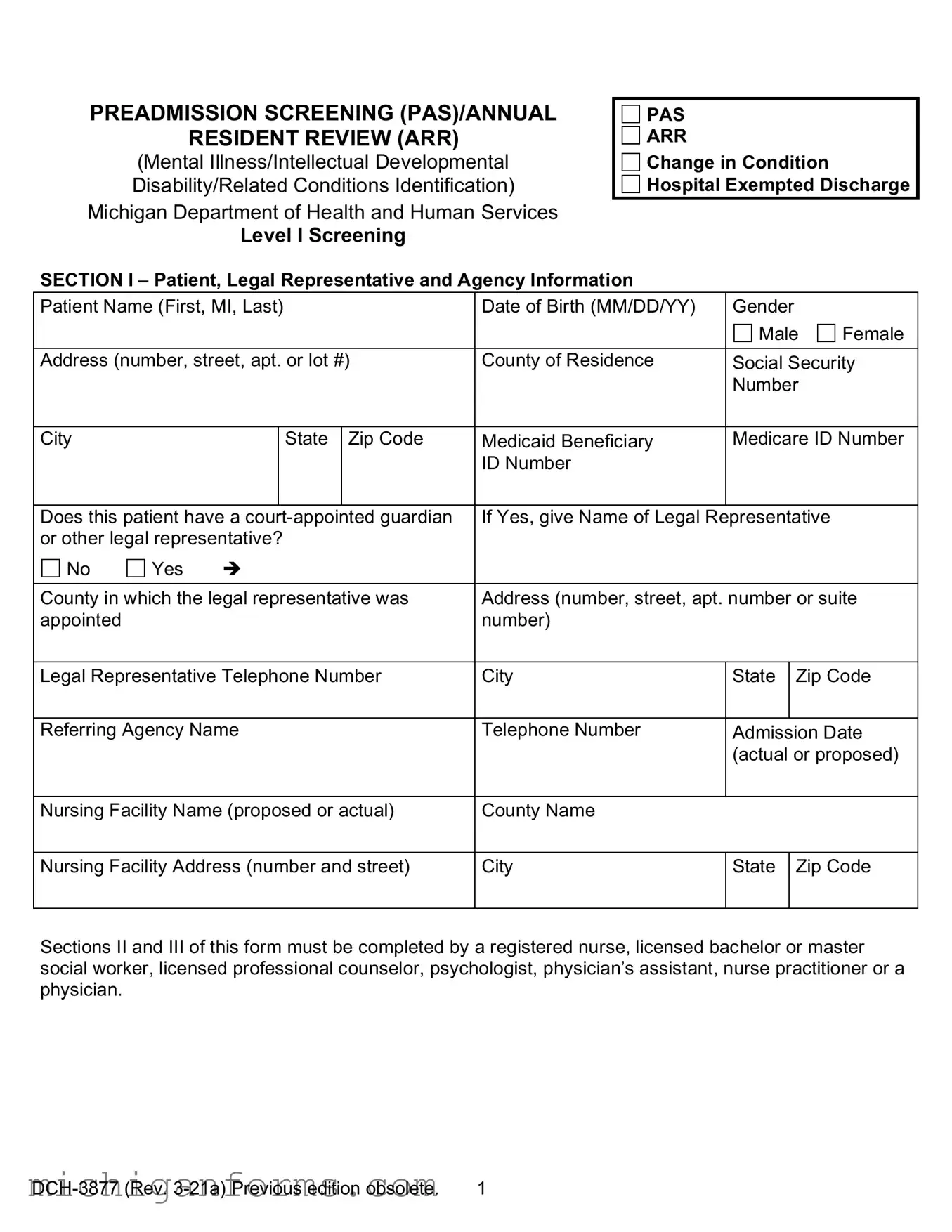
PREADMISSION SCREENING (PAS)/ANNUAL
RESIDENT REVIEW (ARR)
(Mental Illness/Intellectual Developmental
Disability/Related Conditions Identification)
Michigan Department of Health and Human Services
Level I Screening
PAS
ARR
Change in Condition
Hospital Exempted Discharge
SECTION I – Patient, Legal Representative and Agency Information
Patient Name (First, MI, Last) |
Date of Birth (MM/DD/YY) |
Gender |
|
|
|||||
|
|
|
|
|
|
Male |
Female |
||
|
|
|
|
|
|
||||
Address (number, street, apt. or lot #) |
County of Residence |
Social Security |
|||||||
|
|
|
|
|
|
Number |
|
||
|
|
|
|
|
|
|
|
||
City |
|
|
State |
Zip Code |
Medicaid Beneficiary |
Medicare ID Number |
|||
|
|
|
|
|
ID Number |
|
|
|
|
|
|
|
|
|
|
|
|||
Does this patient have a |
If Yes, give Name of Legal Representative |
|
|||||||
or other legal representative? |
|
|
|
|
|
||||
No |
Yes |
|
|
|
|
|
|
||
|
|
|
|||||||
County in which the legal representative was |
Address (number, street, apt. number or suite |
||||||||
appointed |
|
|
|
|
number) |
|
|
|
|
|
|
|
|
|
|||||
Legal Representative Telephone Number |
City |
State |
|
Zip Code |
|||||
|
|
|
|
||||||
Referring Agency Name |
Telephone Number |
Admission Date |
|||||||
|
|
|
|
|
|
(actual or proposed) |
|||
|
|
|
|
|
|
||||
Nursing Facility Name (proposed or actual) |
County Name |
|
|
|
|
||||
|
|
|
|
||||||
Nursing Facility Address (number and street) |
City |
State |
|
Zip Code |
|||||
|
|
|
|
|
|
|
|
|
|
Sections II and III of this form must be completed by a registered nurse, licensed bachelor or master social worker, licensed professional counselor, psychologist, physician’s assistant, nurse practitioner or a physician.
1 |
Patient Name |
Date of Birth (MM/DD/YY) |
|
|
|
|
|
|
|
|
SECTION II – Screening Criteria (All 6 items must be completed.) |
|
|
||
1. |
The person has a current diagnosis of Mental Illness or Dementia (Circle one or |
No |
Yes |
|
|
both) |
|
|
|
2. |
The person has received treatment for Mental Illness or Dementia (within the past |
No |
Yes |
|
|
24 months) (Circle one or both) |
|
|
|
3. |
The person has routinely received one or more prescribed antipsychotic or |
No |
Yes |
|
|
antidepressant medications within the last 14 days. |
|
|
|
4. |
There is presenting evidence of mental illness or dementia, including significant |
No |
Yes |
|
|
disturbances in thought, conduct, emotions, or judgment. Presenting evidence may |
|
|
|
|
include, but is not limited to, suicidal ideations, hallucinations, delusions, serious |
|
|
|
|
difficulty completing tasks, or serious difficulty interacting with others. |
|
|
|
5. |
The person has a diagnosis of an intellectual/developmental disability or a related |
No |
Yes |
|
|
condition including, but not limited to, epilepsy, autism, or cerebral palsy and this |
|
|
|
|
diagnosis manifested before the age of 22. |
|
|
|
6. |
There is presenting evidence of deficits in intellectual functioning or adaptive |
No |
Yes |
|
|
behavior which suggests that the person may have an intellectual/developmental |
|
|
|
|
disability or a related condition. These deficits appear to have manifested before the |
|
|
|
|
age of 22. |
|
|
|
Note: If you check “Yes” to items 1 and/or 2, circle the word “Mental Illness” and/or “Dementia.”
Explain any “Yes”
Note: The person screened shall be determined to require a comprehensive Level II OBRA evaluation if any of the above items are "Yes" UNLESS a physician, nurse practitioner or physician’s assistant certifies on form
SECTION III – CLINICIAN’S STATEMENT: I certify to the best of my knowledge that the above information is accurate.
Clinician Signature |
Date |
Name (type or print) |
|
|
|
Address (number, street, apt. number or suite |
Degree/License |
|
number) |
|
|
City
State
Zip Code
Telephone Number
The Michigan Department of Health and Human Services will not exclude from participation in, deny benefits of, or discriminate against any individual or group because of race, sex, religion, age, national origin, color, height, weight, marital status, gender identification or expression, sexual orientation, partisan considerations, or a disability or genetic information that is unrelated to the person’s eligibility.
AUTHORITY: Title XIX of the Social Security Act
COMPLETION: Is voluntary, however, if NOT completed, Medicaid will not reimburse the nursing facility.
DISTRIBUTION: If any answer to items 1 – 6 in SECTION II is "Yes", send ONE copy to the local Community Mental Health Services Program (CMHSP), with a copy of form
2 |
PREADMISSION SCREENING (PAS)/ANNUAL RESIDENT REVIEW (ARR)
Mental Illness/Intellectual Developmental Disability/Related Conditions Identification
Instructions for Completing Level I Screening
This form is used to identify prospective and current nursing facility residents who meet the criteria for possible mental illness or intellectual/developmental disability, or a related condition and who may be in need of mental health services.
Sections II and III must be completed by a registered nurse, licensed bachelor or master social worker, licensed professional counselor, psychologist, physician’s assistant, nurse practitioner or physician.
Preadmission Screening or Hospital Exempted Discharge: The referral source completing the Level I Screening
Annual Resident Review or Change in Condition: This form must be completed by the nursing facility.
Check the appropriate box in the upper
Section II – Screening Criteria – All 6 items in this section must be completed. The following provides additional explanation of the items.
1.Mental Illness: A current primary diagnosis of a mental disorder as defined in the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders.
Current Diagnosis means that a clinician has established a diagnosis of a mental disorder within the past 24 months. Do NOT mark “Yes” for an individual cited as having a diagnosis "by history" only.
2.Receipt of treatment for mental illness or dementia within the past 24 months means any of the following: inpatient psychiatric hospitalization; outpatient services such as psychotherapy, day program, or mental health case management; or referral for psychiatric consultation, evaluation, or prescription of psychopharmacological medications.
3.Antidepressant and antipsychotic medications mean any currently prescribed medication classified as an antidepressant or antipsychotic, plus Lithium Carbonate and Lithium Citrate.
4.Presenting evidence means the individual currently manifests symptoms of mental illness or dementia, which suggests the need for further evaluation to establish causal factors, diagnosis and treatment recommendations. Further evaluation may need to be completed if evidence of suicidal ideation, hallucinations, delusion, serious difficulty completing tasks or serious difficulty interacting with others.
5.Intellectual/Developmental Disability/Related Condition: An individual is considered to have a severe, chronic disability that meets ALL 4 of the following conditions:
a.It is manifested before the person reaches age 22.
b.It is likely to continue indefinitely.
c.It results in substantial functional limitations in 3 or more of the following areas of major life activity:
3 |
d.It is attributable to:
•Intellectual/Developmental Disability such that the person has significant subaverage general intellectual functioning existing concurrently with deficits in adaptive behavior and manifested during the developmental period;
•cerebral palsy, epilepsy, autism; or
•any condition other than mental illness found to be closely related to Intellectual/ Developmental Disability because this condition results in impairment in general intellectual functioning OR adaptive behavior similar to that of persons with Intellectual/Developmental Disability and requires treatment or services similar to those required for these persons.
6.Presenting evidence means the individual manifests deficits in intellectual functioning or adaptive behavior, which suggests the need for further evaluation to determine the presence of a developmental disability, causal factors, and treatment recommendations. These deficits appear to have manifested before the age of 22.
Note: When there are one or more "Yes" answers to items 1 – 6 under SECTION II, complete form
4 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Law | The DCH-3877 form is governed by Public Act 280 of 1939, which establishes the legal framework for the operation of the Michigan Department of Community Health. |
| Purpose of the Form | The form is used for Preadmission Screening (PAS) and Annual Resident Review (ARR) for individuals with Mental Illness/Developmental Disability, aiming to identify those in need of mental health services in nursing facilities, hospitals, and community mental health services programs. |
| Completion Requirement | Completion of the DCH-3877 form is voluntary; however, it is required for Medicaid program payment desires, ensuring that individuals receive the appropriate care and services funded by Medicaid. |
| Significant Changes | Revisions to the form reflected updates including the change to the Diagnostic and Statistical Manual of Mental Disorders to the 4th edition (DSM IV), the renaming of certain healthcare entities, and adjustments in language from "exception" to "exemption". |
Guidelines on Utilizing Michigan Dch 3877
Filling out the Michigan DCH-3877 form is a crucial step for ensuring that individuals who are either entering or currently residing in nursing facilities receive the appropriate assessment regarding mental illness or developmental disability. This process helps in identifying the need for specialized mental health services. The guidelines below are designed to simplify the form completion process. By following these steps carefully, you can ensure that the form is accurately filled out and submitted correctly, facilitating the necessary evaluations and interventions for the individual in question.
- Begin by selecting the appropriate checkbox at the top of the form to indicate whether this is for a Preadmission Screening (PAS) or an Annual Resident Review (ARR).
- Under Section I, fill in the patient's full name, date of birth, and indicate their gender by checking the appropriate box.
- Provide the patient's complete address, including the number and street, city, state, ZIP code, and county of residence.
- Enter the patient's Social Security Number, Medicaid Beneficiary ID Number, and Medicare ID Number if available.
- If the patient has a court-appointed guardian or other legal representative, check "YES" and provide the name of the guardian or legal representative, the county in which the guardian was appointed, their complete address, and telephone number.
- Fill in the referring agency name, telephone number, and the admission date (actual or proposed).
- Indicate the proposed or actual nursing facility name, its county name, facility address, city, state, and ZIP code.
- In Section II, answer all six screening criteria questions by checking "YES" or "NO." If "YES" is answered for items 1 and/or 2, circle the condition being screened for—either "mental illness" or "dementia."
- For any "YES" answer given in Section II, provide an explanation of the evidence or circumstances that led to this answer.
- In Section III, the clinician's statement requires the clinician to certify the accuracy of the information provided. The clinician must sign and date the form, then print their name, degree/license, address, and telephone number.
- Remember to check the requirements for a DCH-3878 form completion if you answered "YES" to any items in Section II. This is necessary to establish exemption criteria and should accompany the DCH-3877 when necessary.
- Upon completing the form, distribute copies accordingly: send one copy to the local Community Mental Health Services Program (CMHSP), retain the original in the patient's record, and ensure a copy is provided to the patient or their authorized representative.
Accurate and thorough completion of the Michigan DCH-3877 form is essential for ensuring that individuals in nursing facilities receive the care and services they need. This document is not only a requirement but a tool to help healthcare providers offer the best support for those with mental illness or developmental disabilities within the nursing facility setting.
Crucial Points on This Form
What is the purpose of the Michigan DCH-3877 form?
The DCH-3877 form serves a critical role in the healthcare system by helping to identify individuals entering nursing facilities who may have mental illness or developmental disabilities. This screening ensures that persons with these conditions receive the appropriate mental health services they need. Specifically, it's used for both preadmission screening and annual resident review processes to ensure continuous, comprehensive care.
Who is required to complete the DCH-3877 form?
This form must be completed by healthcare professionals who are equipped with the requisite knowledge and skills to accurately assess the patient's condition. These professionals include registered nurses, certified or registered social workers, psychologists, physician’s assistants, or physicians. This ensures the assessment is thorough and based on a detailed understanding of the patient's medical and psychological needs.
What kind of information needs to be provided on the DCH-3877 form?
- Patient, Guardian, and Agency Information: Basic details about the patient, including name, birth date, gender, contact information, and guardian details, if applicable.
- Screening Criteria: Answering questions related to the patient's mental health history, treatments, and current medications to identify the need for a mental illness or developmental disability evaluation.
- Clinician's Statement: A certification by the clinician that the information provided is accurate to the best of their knowledge.
What happens if the screening on the DCH-3877 form indicates a need for further evaluation?
If the screening indicates potential mental illness or developmental disability, a comprehensive Level II OBRA screening is required unless a physician certifies that the patient meets exemption criteria on form DCH-3878. This process ensures that patients receive the level of care and evaluation necessary for their specific conditions, promoting personalized and effective healthcare interventions.
How can providers obtain the DCH-3877 and DCH-3878 forms?
Providers can order the DCH-3877 and DCH-3878 forms from the Michigan Department of Community Health, Forms Distribution, located in the Lewis Cass Building, 320 S. Walnut Street, Lansing, Michigan. Additionally, these forms are available for download from the Michigan Department of Community Health website, offering easy access for healthcare providers to facilitate the screening process.
Common mistakes
One common mistake when filling out the Michigan DCH-3877 form is not fully completing the Patient, Guardian, and Agency Information section. This section collects essential details about the patient, guardian, and the referring agency. Omitting information like the Medicaid Beneficiary ID Number or the correct contact details for the guardian can lead to delays in the screening process.
Another error involves misunderstanding the role of the professional completing the form. The DCH-3877 must be filled out by a registered nurse, certified or registered social worker, psychologist, physician’s assistant, or physician. Sometimes, those without the proper credentials attempt to complete the form, which results in the need for resubmission and unnecessary delays.
Additionally, individuals sometimes inaccurately answer the screening criteria questions in Section II. These questions are crucial for determining the need for a comprehensive Level II screening. Incorrectly circling "YES" or "NO" or failing to circle the specific condition being screened for—mental illness or dementia—can lead to incorrect routing of the form.
Failing to clearly explain any "YES" responses in Section II is another mistake. When a "YES" response is provided, a clear explanation is required to guide the appropriate follow-up. Without this explanation, it can be difficult for the reviewing agency to determine the next steps.
When it comes to Section III, the Clinician’s Statement, a frequent oversight is failing to include the clinician's name, degree/license, and contact information. This section is vital for verifying the authenticity of the screening and for follow-up if there are questions about the form. Incomplete or illegible information here can invalidate the form.
Overlooking the requirement for a physician to certify the form DCH-3878 if any exemptions are being requested based on the outcomes of the DCH-3877 form is another common mistake. This step is critical when an exemption is sought, and missing this step can result in the form being returned for proper completion.
Sometimes, individuals neglect to send a copy of the completed form to the local Community Mental Health Services Program (CMHSP) when a "YES" answer requires it, as detailed in the distribution instructions. This oversight can prevent necessary mental health evaluations and services from being initiated.
Not retaining the original form in the patient's record at the nursing facility, as required, is a procedural error that can affect future care and compliance with state health regulations. This document serves as an important part of the patient’s medical record, showing that proper screening was conducted.
Lastly, a common mistake is not understanding the distinctions between the criteria for mental illness and developmental disability, leading to inappropriate checks in Section II. This misunderstanding can misguide the screening process, delaying appropriate care or misallocating resources.
Documents used along the form
When working with the Michigan DCH-3877 form, which is central to the process of Preadmission Screening and Annual Resident Review (PASARR) for patients dealing with mental illness or developmental disabilities, various other documents might also come into play to ensure comprehensive assessment and regulatory compliance. These documents often supplement the DCH-3877 form, each serving a specific purpose in the broader context of patient care and facility administration.
- Michigan DCH-3878 Form: This form, also referenced in the bulletin, is used alongside the DCH-3877 for certifying exemptions for individuals with dementia or in a coma. It helps in distinguishing those who require a comprehensive Level II screening from those who do not, based on specific criteria.
- Doctor’s Certification: A doctor's written certification may be required in addition to the screening forms to verify the medical conditions of the individual. This document provides a professional opinion on the patient's health status, diagnoses, and the necessity of specialized care or services.
- Guardianship Documents: If the individual has a court-appointed guardian or legal representative, the relevant legal documents confirming guardianship are necessary. These documents establish the legal authority of the representative to make decisions on behalf of the patient.
- Medical History Records: Comprehensive medical history records provide background information crucial for completing the DCH-3877 form. These records include previous diagnoses, treatments, medications, and any other relevant medical interventions.
- Medicare or Medicaid Documentation: Since the PASARR process affects Medicaid services, it’s essential to have current Medicare or Medicaid documentation for the individual. This ensures that billing and eligibility issues are properly addressed.
- Advanced Directives: Advanced healthcare directives or living wills may also be relevant in the context of completing the PASARR process. These documents outline the patient's preferences regarding healthcare decisions, which can be crucial for planning care and services.
In conclusion, the DCH-3877 form does not stand alone in the assessment and admission processes of individuals with mental illness or developmental disabilities. The coordination of various forms and documents ensures a holistic approach to determining the appropriate care setting for each individual, aligning with state regulations and healthcare standards. Each document contributes to a comprehensive understanding of the patient's needs, thereby facilitating informed decisions about their care and support services.
Similar forms
The Uniform Assessment System for New York (UAS-NY) form is similar to the Michigan DCH-3877 form in that both are designed to assess the needs of individuals requiring long-term care services. They collect patient information, including health conditions and living situations, to determine the best course of care and services.
The InterRAI Home Care (HC) Assessment Form is also similar to the DCH-3877 form as it focuses on evaluating the mental, physical, and functional status of individuals to ensure that home care services meet their specific needs, similar to the PAS/ARR process for nursing facility admissions.
California's Pre-Admission Screening and Resident Review (PASRR) Level I Form resembles the DCH-3877. Both forms are part of a PASRR process, focusing on screening individuals for mental illness or intellectual disabilities before nursing facility admission, ensuring appropriate placement and care services.
The Minimum Data Set (MDS) 3.0 used in nursing facilities nationwide has similarities to the DCH-3877 form. While the MDS is more comprehensive, both forms assess the health status of residents to aid in care planning and to ensure residents' needs are met through appropriate services.
Ohio's ODM 3622 Form (PASRR Mental Illness and Intellectual Disability or Related Conditions Screening Form) is akin to Michigan's DCH-3877, as both are dedicated to the identification of mental illness or developmental disability in individuals seeking admission to nursing facilities. Each form requires detailed information about the individual's diagnosis, treatment, and medication history to support the screening process.
The Texas Health and Human Services Commission's (HHSC) PASRR Evaluation (PE) Form shares its purpose with the DCH-3877 form by identifying individuals who may require specialized services due to mental illness or an intellectual disability. Both aim to ensure that individuals receive care in the most appropriate setting according to their needs.
The Resident Assessment Instrument (RAI) MDS 2.0, precursor to the MDS 3.0, was similar to the DCH-3877 in providing a framework for evaluating the care needs of residents in long-term care settings. Both documents gather critical information about the resident's mental, physical, and psychological condition, which helps in developing a personalized care plan.
Dos and Don'ts
When tackling the Michigan DCH-3877 form, an essential document for those involved in the care of individuals with possible mental illness or developmental disabilities, it's crucial to navigate with precision and clarity. Here are eight essential dos and don'ts to guide you through the process effectively.
- Do ensure that the form is completed by a qualified professional. This includes a registered nurse, certified or registered social worker, psychologist, physician’s assistant, or physician, as specified in the form's instructions.
- Do answer all questions with accuracy. This form assesses the need for a comprehensive Level II OBRA screening, making precision critical.
- Do circle the correct condition (mental illness or dementia) when a "YES" response is given to questions under Section II related to current diagnoses and treatment received within the past 24 months.
- Do provide detailed explanations for any "YES" answer in Section II to offer clear evidence and justification for the responses given.
- Don't skip over questions or leave sections incomplete. Each question is designed to determine the necessity for further evaluation and care, making comprehensive responses important.
- Don't check "YES" for a diagnosis by history only. Make sure a current primary diagnosis aligns with the criteria defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM IV).
- Don't forget to attach a copy of the DCH-3878 form if an exemption is requested. This is crucial for establishing exemption criteria for dementia or a state of coma.
- Don't overlook the distribution requirements. Remember to send a copy to the local Community Mental Health Services Program (CMHSP) and retain the original form in the patient's record, ensuring a copy also goes to the patient or authorized patient representative.
By adhering to these guidelines, you can navigate the intricacies of the Michigan DCH-3877 form with confidence, ensuring that necessary screenings and exemptions are accurately identified and processed. This careful attention to detail not only complies with the procedural requirements but also significantly contributes to the quality of care provided to individuals with mental illness or developmental disabilities.
Misconceptions
Michigan DCH-3877 form is surrounded by several misconceptions that sometimes lead to misunderstandings or misuse. Understanding these misconceptions and clarifying the facts is essential for all providers and interested parties to ensure they are properly completing and using the form.
- Misconception #1: The DCH-3877 form is only intended for nursing facilities.
While nursing facilities are a major user of the form, it is also crucial for hospitals and community mental health services programs. The form serves as a critical tool in the preadmission screening and annual resident review process for individuals with mental illness or developmental disabilities.
- Misconception #2: Any healthcare professional can complete the DCH-3877 form.
The form must be completed by professionals with specific qualifications, such as registered nurses, certified or registered social workers, psychologists, physician's assistants, or physicians. This ensures that the assessment and the provided information are accurate and reliable.
- Misconception #3: The DCH-3877 form is optional.
Completion of the form is voluntary; however, it is required if Medicaid program payment is desired. This underscores the form's importance in streamlining Medicaid's support for patients with mental health and developmental disabilities.
- Misconception #4: There are no significant changes in the revised versions of the forms.
The bulletin specifically notes that the forms have been revised to more appropriately reflect their usage, including the change of certain terms and diagnostic criteria to align with current practices and standards.
- Misconception #5: The form is complicated and time-consuming to fill out.
While comprehensive, the DCH-3877 form is designed to be straightforward and efficient in gathering necessary information. The guidelines provided with the form aim to facilitate its completion without causing unnecessary confusion or delay.
- Misconception #6: The DCH-3877 and DCH-3878 forms serve the same purpose.
Although related, the DCH-3877 form is used for the preadmission screening or annual resident review, while the DCH-3878 form is specifically for the certification of mental illness/developmental disability exemption criteria. Each plays a unique role in the patient evaluation and admission process.
- Misconception #7: A positive screening result on the DCH-3877 automatically disqualifies the individual from nursing facility admission.
A "yes" answer to any of the screening questions requires a comprehensive Level II OBRA screening but does not automatically disqualify the individual from admission. A physician can certify on form DCH-3878 that the person meets an exemption criteria, allowing for further evaluation and consideration.
Clarifying these misconceptions is crucial for ensuring that individuals who need mental health or developmental disability services receive appropriate care and support in a timely manner. Providers equipped with the correct information can navigate the process more effectively, ultimately benefiting the patients they serve.
Key takeaways
Filling out and using the Michigan DCH-3877 form requires detailed attention to ensure compliance with Medicaid guidelines and proper care planning for individuals with potential mental illness or developmental disabilities. Here are some key takeaways to consider:
- The DCH-3877 form is essential for identifying both prospective and current nursing facility residents who might have mental illness or developmental disabilities and could require specialized mental health services. This form must be filled out by professionals such as registered nurses, certified or registered social workers, psychologists, physician assistants, or physicians.
- It is a requirement to complete the DCH-3877 as part of the discharge planning process by hospitals or by physicians who intend to admit an individual to a nursing facility from non-acute care settings. There are specific sections for preadmission screening (PAS) and annual resident review (ARR), which are critical for ongoing resident assessment.
- For a comprehensive understanding of a patient's condition, the form includes a section on screening criteria that cover diagnoses of mental illness or dementia, recent treatment for these conditions, current prescriptions, and evidence of significant disturbances or disabilities. This part helps in determining the necessity for a more detailed Level II screening.
- When filling out the form, it's important not to mark “YES” for an individual cited as having a diagnosis "by history" only. Accurate and current diagnostic information is crucial for correctly assessing the need for special care or exemptions.
- If the screening results in any "YES" answers to the specified items, a DCH-3878 form must be completed to establish if the patient meets the exemption criteria for dementia, a state of coma, or exempted hospital discharge. This step ensures proper documentation and compliance with Medicaid requirements.
Providers need to follow these guidelines carefully to ensure that patients are accurately assessed and receive the appropriate level of care. Completing these forms accurately and timely not only supports patient well-being but also enables facilities to meet regulatory requirements and secure necessary funding.
Popular PDF Templates
Michigan Sales and Use Tax Login - Businesses provide information on their Michigan sales, both taxable and nontaxable, to determine economic presence within the state.
Motion to Set Aside - Standardized Michigan judicial document for addressing failures to plead or otherwise defend in court.
Annulment in Michigan Time Limit - The form serves as an official state record, falling under the authority of specific Michigan legislation.