Bfs 108 Michigan PDF Form
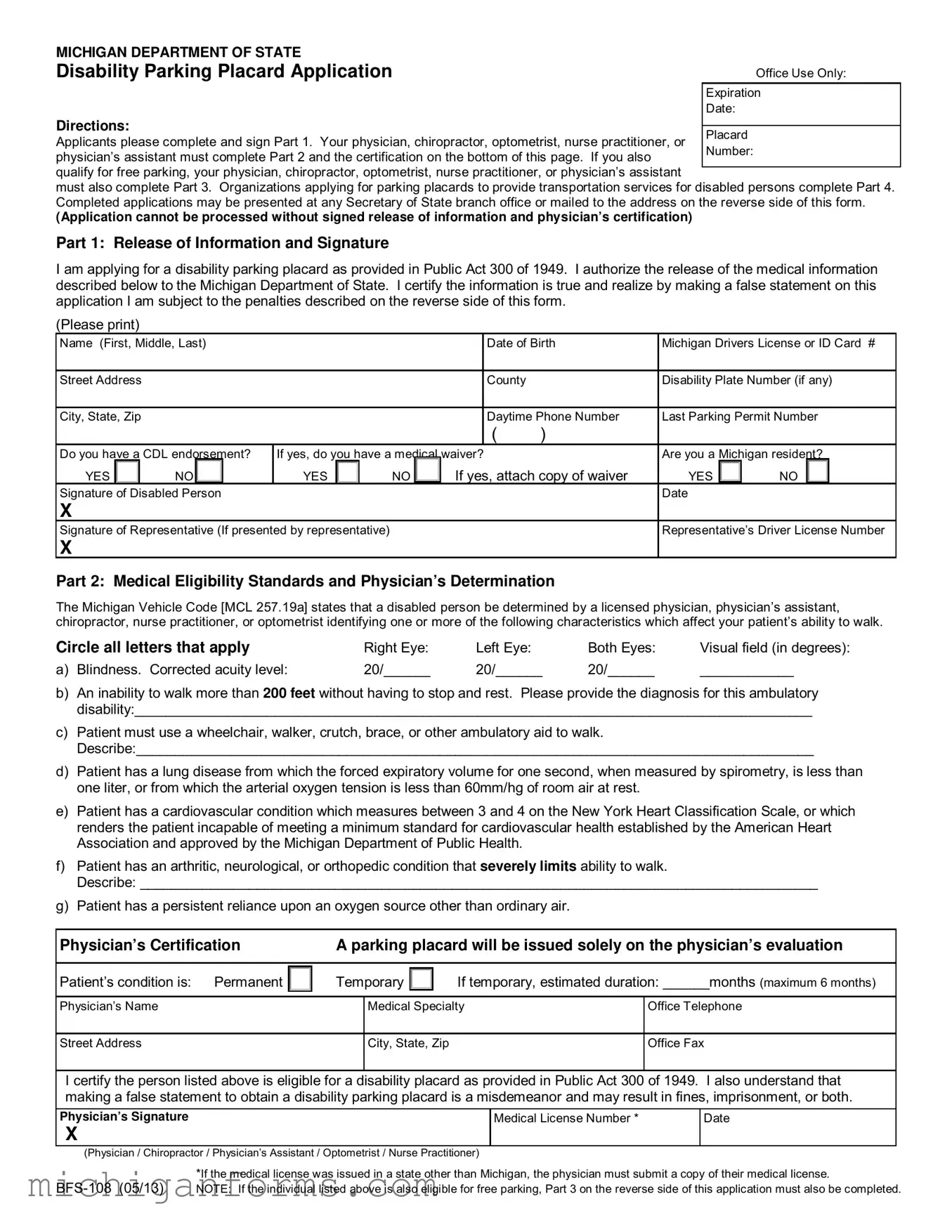
Navigating through the requirements and procedures to obtain a disability parking placard in Michigan is made clearer with the Bfs 108 Michigan form. This essential document, provided by the Michigan Department of State, streamlines the process for individuals seeking accommodations for disability parking. The form is divided into distinct sections, catering to both individual applicants and organizations providing transportation services for disabled persons. Applicants must furnish details about their disability and undergo certification by a healthcare professional—such as a physician, chiropractor, optometrist, nurse practitioner, or physician’s assistant—to establish medical eligibility. An added layer of assistance is offered to those who qualify for free parking, requiring further certification regarding the severity of the disability and its impact on mobility. The form also outlines the responsibilities and legal implications for applicants, underscoring the importance of truthfulness and accuracy in the application process. Organizations looking to support disabled persons through transportation services must complete a separate section to request disability parking placards, ensuring they meet state guidelines and maintain the integrity of the service provided. Penalties for misuse or fraudulent applications are highlighted, emphasizing the legal standards upheld by the Michigan Vehicle Code. By completing and submitting the Bfs 108 form, applicants and organizations take a significant step toward receiving the necessary accommodations for disability parking, marking an important juncture in the pursuit of mobility and independence.
Preview - Bfs 108 Michigan Form
MICHIGAN DEPARTMENT OF STATE |
|
Disability Parking Placard Application |
Office Use Only: |
|
Expiration |
|
Date: |
Directions:
Applicants please complete and sign Part 1. Your physician, chiropractor, optometrist, nurse practitioner, or physician’s assistant must complete Part 2 and the certification on the bottom of this page. If you also qualify for free parking, your physician, chiropractor, optometrist, nurse practitioner, or physician’s assistant
must also complete Part 3. Organizations applying for parking placards to provide transportation services for disabled persons complete Part 4. Completed applications may be presented at any Secretary of State branch office or mailed to the address on the reverse side of this form.
(Application cannot be processed without signed release of information and physician’s certification)
Part 1: Release of Information and Signature
I am applying for a disability parking placard as provided in Public Act 300 of 1949. I authorize the release of the medical information described below to the Michigan Department of State. I certify the information is true and realize by making a false statement on this application I am subject to the penalties described on the reverse side of this form.
(Please print)
Name (First, Middle, Last) |
|
|
|
|
|
|
Date of Birth |
Michigan Drivers License or ID Card # |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
|
|
|
County |
|
Disability Plate Number (if any) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City, State, Zip |
|
|
|
|
|
|
|
|
|
Daytime Phone Number |
Last Parking Permit Number |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
Do you have a CDL endorsement? |
If yes, do you have a medical |
waiver? |
|
Are you a Michigan resident? |
||||||||||||||
YES |
|
|
NO |
|
|
YES |
|
|
NO |
If yes, attach copy of waiver |
YES |
|
NO |
|
|
|||
Signature of Disabled Person |
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Signature of Representative (If presented by representative) |
|
|
|
|
|
Representative’s Driver License Number |
||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Part 2: Medical Eligibility Standards and Physician’s Determination
The Michigan Vehicle Code [MCL 257.19a] states that a disabled person be determined by a licensed physician, physician’s assistant, chiropractor, nurse practitioner, or optometrist identifying one or more of the following characteristics which affect your patient’s ability to walk.
Circle all letters that apply |
Right Eye: |
Left Eye: |
Both Eyes: |
Visual field (in degrees): |
a) Blindness. Corrected acuity level: |
20/______ |
20/______ |
20/______ |
____________ |
b)An inability to walk more than 200 feet without having to stop and rest. Please provide the diagnosis for this ambulatory disability:_______________________________________________________________________________________
c)Patient must use a wheelchair, walker, crutch, brace, or other ambulatory aid to walk.
Describe:_______________________________________________________________________________________
d)Patient has a lung disease from which the forced expiratory volume for one second, when measured by spirometry, is less than one liter, or from which the arterial oxygen tension is less than 60mm/hg of room air at rest.
e)Patient has a cardiovascular condition which measures between 3 and 4 on the New York Heart Classification Scale, or which renders the patient incapable of meeting a minimum standard for cardiovascular health established by the American Heart Association and approved by the Michigan Department of Public Health.
f)Patient has an arthritic, neurological, or orthopedic condition that severely limits ability to walk.
Describe: _______________________________________________________________________________________
g)Patient has a persistent reliance upon an oxygen source other than ordinary air.
Physician’s Certification |
|
A parking placard will be issued solely on the physician’s evaluation |
||||
|
|
|
|
|
|
|
Patient’s condition is: Permanent |
|
Temporary |
|
|
If temporary, estimated duration: ______months (maximum 6 months) |
|
|
|
|
||||
|
|
|
|
|
|
|
Physician’s Name |
|
Medical Specialty |
Office Telephone |
|||
|
|
|
|
|
|
|
Street Address |
|
City, State, Zip |
|
Office Fax |
||
I certify the person listed above is eligible for a disability placard as provided in Public Act 300 of 1949. I also understand that making a false statement to obtain a disability parking placard is a misdemeanor and may result in fines, imprisonment, or both.
Physician’s Signature
X
(Physician / Chiropractor / Physician’s Assistant / Optometrist / Nurse Practitioner)
Medical License Number *
Date
*If the medical license was issued in a state other than Michigan, the physician must submit a copy of their medical license.
Part 3: Free Parking Application And Physician’s Certification
The free parking application is completed only when the applicant qualifies for free parking. To qualify, your patient must be a Michigan licensed driver, have an ambulatory disability described in Part 2, and also have one of the following conditions. Economic need is not a consideration.
Circle all letters that apply:
a)The patient cannot insert coins or tokens in a parking meter or cannot accept a ticket from a parking lot machine due to a lack of fine motor control of both hands.
b)The patient cannot reach above their head to a height of 42 inches from the ground, due to a lack of finger, hand, or upper extremity strength or mobility.
c)The patient cannot approach a parking meter due to use of a wheelchair or other ambulatory device.
d)The patient cannot walk more than twenty feet due to an orthopedic, cardiovascular, or lung condition in which the degree of debilitation is so severe that it almost completely impedes the patient’s ability to walk. (A condition requiring applicant to rest after walking twenty feet when not using a wheelchair or other ambulatory device.)
I certify the person listed on the front of this application is also eligible for free parking as provided in state law [MCL 257.675]. I under- stand that making a false statement to obtain a free parking sticker is a misdemeanor and may result in fines, imprisonment, or both.
Physician’s signature: X |
|
Date |
|
|
|
(Physician / Chiropractor / Physician’s Assistant / Optometrist / Nurse Practitioner) |
|
_________________________________________________________________________________________________
Part 4: Organization Request For Disability Parking Placards
(Please print)
Name of Organization
County
Telephone Number
( )
Street Address
City, State, Zip
Describe the transportation services your organization provides to persons with disabilities:
Number of disability placards you are requesting: ________ (No more then 1 per vehicle used to transport clients.)
I am applying for a disability parking placard as provided in Public Act 300 of 1949 and certify the above information is true.
Signature of Organization Officer |
Printed Name of Organization Officer |
Date |
X |
|
|
Organization Officer’s Driver License Number |
Position (Title) with Organization |
|
|
|
|
Note: If the organization ceases to provide specialized services to disabled persons, the parking placard must be returned to the Secretary of State for cancellation.
__________________________________________________________________________________________________
Penalties
Michigan Vehicle Code Section 257.675 Prohibits:
●Using a disability parking placard to park in a designated parking space unless the disabled person is driving or being transported.
●Altering, modifying, or selling a disability parking placard or free parking sticker.
●Copying or forging, or using a copied or forged disability parking placard or free parking sticker.
●Making a false statement to obtain a disability parking placard or free parking sticker, or committing a deception or fraud on a medical statement attesting to a disability.
●Knowingly using or displaying a disability parking placard that has been canceled by the Secretary of State.
A violation is a misdemeanor and punishable by a fine up to $500 or imprisonment for up to 30 days, or both. A law enforcement officer may immediately confiscate a disability parking placard for improper use.
__________________________________________________________________________________________________
Return completed applications to any |
Michigan Department of State |
Secretary of State branch office or mail to: |
|
|
PO Box 30764 |
|
Lansing, MI 48918 |
If you have any questions regarding disability parking placards, please call
Authority granted under Pubic Act 300 of 1949, as amended.
Form Characteristics
| Fact Name | Detail |
|---|---|
| Purpose of the Form | The BFS-108 form is used for applying for a disability parking placard in Michigan. |
| Governing Law | This application process is governed by Public Act 300 of 1949. |
| Eligibility Criteria | Eligible conditions include visual impairments, difficulties in walking specific distances without rest, reliance on ambulatory aids, certain lung diseases, cardiovascular conditions, severe arthritic, neurological, or orthopedic conditions, or dependence on an external oxygen source. |
| Medical Certification Requirement | Medical eligibility must be certified by a licensed physician, physician’s assistant, chiropractor, nurse practitioner, or optometrist. |
| Penalties for Misuse | Misuse of the disability parking placard can lead to fines up to $500, imprisonment for up to 30 days, or both. Violations include using a placard improperly, altering or selling a placard, making a false statement to obtain a placard, or using a placard that has been canceled. |
Guidelines on Utilizing Bfs 108 Michigan
Once the decision is made to apply for a Michigan Disability Parking Placard, a critical step to ensure access to parking accommodations begins. Filling out the BFS-108 Michigan form properly is key to obtaining the necessary placard. Different sections of the form require attention from both the applicant and a certified healthcare provider. Follow these instructions carefully to navigate the process smoothly. After completing and submitting this form, remember, it can be taken to any Secretary of State branch office or mailed directly. Now, let’s walk through the necessary steps to complete the form.
- Part 1: Begin with your personal information. Print your full name, date of birth, driver’s license or ID card number, and complete address including county. Also, provide details about any previous parking permits, including the last one issued, and specify if you have a CDL endorsement or require a medical waiver. Answer the residency question and then sign and date the form. If a representative is assisting, they must also sign and include their driver’s license number.
- Part 2: This section must be completed by a licensed healthcare professional (physician, chiropractor, optometrist, nurse practitioner, or physician's assistant). It requires them to detail the medical eligibility standards met by the applicant. Conditions that affect the applicant’s ability to walk must be thoroughly described, and the healthcare provider must circle specific characteristics that apply. The provider then needs to mark if the condition is permanent or temporary, sign, provide their medical license number, office contact information, and date the certification. If the medical license is issued outside Michigan, a copy must be attached.
- Part 3 (if applicable): If the applicant also qualifies for free parking, this section should be filled out by the same healthcare professional. They need to identify the specific conditions that qualify the applicant for this benefit, sign, and date this section of the form.
- Part 4: This section is reserved for organizations applying for parking placards to transport persons with disabilities. The organization must provide its name, address, contact information, a description of its services, the number of placards requested, and an authorized officer must sign and date the form.
After the form is fully completed, review it to make sure all sections applicable to your situation have been accurately filled out. Incorrect or incomplete forms may delay the process. Finally, you can submit this form either in person at a Secretary of State branch office or mail it to the address provided on the form. Remember, the application cannot be processed without the signed release of information and a physician’s certification. Regularly follow up to check the status and be ready to provide any additional information if requested.
Crucial Points on This Form
What is the BFS 108 Michigan form used for?
The BFS 108 Michigan form is an application for obtaining a disability parking placard in Michigan. This placard allows individuals with disabilities to park in designated parking spaces, making access to buildings and facilities easier. The form is part of the process for people with certain medical conditions to apply for either temporary or permanent disability parking privileges. It requires certification from a healthcare professional to confirm the individual's eligibility based on their mobility challenges or visual impairments.
Who can complete the medical certification on the BFS 108 form?
The medical certification section of the BFS 108 form must be completed by a licensed healthcare provider. Eligible professionals include a physician, chiropractor, optometrist, nurse practitioner, or physician’s assistant. These professionals must examine the applicant and verify their disability affects their ability to walk or requires that they rely on a wheelchair, crutch, or other ambulatory aids. They also determine if the disability is temporary or permanent.
Can organizations apply for disability parking placards?
Yes, organizations that provide transportation services for disabled persons can apply for disability parking placards. Part 4 of the BFS 108 form is specifically designed for such organizations. They are required to detail the transportation services offered to persons with disabilities and specify the number of placards needed, with the stipulation that one placard is issued per vehicle utilized for client transport. The signature of an organization officer is also required to certify the accuracy of the information provided.
What are the consequences of misusing a disability parking placard?
Misusing a disability parking placard is taken very seriously in Michigan. Actions considered misuse include parking in a designated space without the disabled person being transported, altering or selling a placard, copying or forging a placard, or making false statements to obtain one. Such violations are classified as misdemeanors and are punishable by fines up to $500, imprisonment for up to 30 days, or both. Additionally, law enforcement officers have the authority to immediately confiscate a placard if it is being improperly used.
How can one return or renew a disability parking placard in Michigan?
For returning or renewing a disability parking placard, individuals or organizations should contact the Michigan Department of State, either through a Secretary of State branch office or by mail. If renewing, the process will likely require a new application form to be completed, including another medical certification for temporary conditions. Permanent placards may have a renewal process that varies, so it's important to check the latest requirements by calling the provided contact number or visiting the Secretary of State's website. Should an organization cease to provide services to disabled persons, the placard must be returned for cancellation.
Common mistakes
Filling out the BFS 108 Michigan form, a crucial document for those in need of a disability parking placard, often involves a series of common errors that can delay or complicate the application process. Understanding and avoiding these mistakes is key to a smoother and faster approval.
Firstly, applicants frequently forget to complete all required sections of Part 1 or to sign the form, a simple but critical step. Without a signature, the application is deemed incomplete, and the Michigan Department of State cannot process it. This oversight, though small, leads to unnecessary delays.
Another frequent mistake is not accurately providing the Michigan Drivers License or ID Card number. This piece of information is vital for verifying the identity of the applicant and ensuring they are entitled to the benefits being applied for. An incorrect or missing number can halt the process.
Many applicants also falter when it comes to detailing their disability in Part 2 of the form. The omission of specific diagnosis or descriptions of one's disability can lead to ambiguity, making it difficult for the reviewing officials to determine eligibility. It is imperative that this section is filled out meticulously and completely.
In addition to the above, a common pitfall is not ensuring that the healthcare provider completes their section fully and accurately. This section validates the disability and is essential for the application to be considered. Incomplete or vague information from the physician or healthcare provider can result in the application being returned or denied.
Another mistake involves misunderstanding or not completing Part 3, the free parking application section, correctly. This applies only to those who meet specific criteria outlined in the form. Applicants often either overlook this section when they qualify or fill it out without meeting the criteria, leading to confusion during the processing of their application.
Organizations applying for parking placards via Part 4 sometimes fail to describe adequately the transportation services they provide to persons with disabilities. This description is crucial for the Department of State to assess the necessity and number of placards an organization is entitled to. Vague or incomplete descriptions may result in fewer placards being issued than needed.
Applicants and healthcare providers alike frequently overlook the necessity of signing the application. These signatures are a mandatory part of the application process, serving as a certification of truthfulness and accuracy of the information provided. An unsigned application is considered incomplete and cannot be processed.
Additionally, applicants sometimes submit the form without attaching required documents, such as a copy of the medical waiver for CDL endorsement holders. This omission can halt the application processing until all necessary documentation is received.
Some applicants mistakenly believe economic need is a consideration for free parking eligibility and may misrepresent their conditions to qualify. This misunderstanding not only delays the process but can also lead to penalties for false statements.
Lastly, failing to contact the Secretary of State's office with questions or for clarification on certain sections of the application can lead to errors. Assistance is available, and taking advantage of it can help avoid common mistakes and ensure the application is filled out correctly the first time around.
By being aware of and avoiding these common mistakes, applicants can streamline their experience in obtaining a disability parking placard in Michigan, ensuring prompt access to the benefits and accommodations they need.
Documents used along the form
When someone completes the BFS-108 Michigan form for a disability parking placard, several other forms and documents might be relevant to their situation. Accessibility and ease of mobility are fundamental, and understanding the associated paperwork can help streamline the process, ensuring that individuals receive the support and resources they need. Here's a quick overview of some other forms and documents that are often paired with the BFS-108 form:
- Proof of Identity Document: This could be a driver's license, state ID, or any official document that verifies the applicant's identity.
- Medical Documentation: Detailed records or a letter from a healthcare provider that outlines the nature of the disability, offering evidence to support the application for a parking placard.
- Vehicle Registration: If a permanent placard is being sought, vehicle registration documents might be required to link the placard to the applicant's vehicle.
- Secretary of State (SOS) Forms: Additional forms from the SOS office, potentially for renewing or replacing a lost placard.
- Free Parking Sticker Application: For those who qualify, this application is necessary to obtain a sticker that allows for free parking.
- Change of Address Form: If the applicant has recently moved, this form will help ensure that the placard is sent to the correct address.
- License Plate Application: For those who prefer or also need disability license plates, a separate application is required.
- Appeal Forms: If an application is denied, appeal forms are necessary to contest the decision.
Handling these documents can seem overwhelming, but they're all designed to ensure that individuals with disabilities have the access and accommodations they need. Each form plays a part in assembling a comprehensive picture of the applicant's needs, making it easier for authorities to offer the appropriate support. Whether someone is applying for a placard for the first time or renewing an existing one, these documents ensure that the process is as smooth and efficient as possible.
Similar forms
Handicap Parking Application Forms from Other States: Like the BFS 108 Michigan form, many states have their own versions of disability parking placard applications. These forms typically require personal information, the nature of the disability, and a healthcare professional’s certification, similar to Michigan's requirements. The primary similarity lies in the process: an application filled out by the applicant, medical certification by a professional, and submission protocols.
Temporary Disability Placard Applications: Some states differentiate between permanent and temporary disability parking applications. The BFS 108 form covers both types, asking the medical professional to indicate whether the disability is temporary or permanent and, if temporary, the estimated duration of the condition. This dual functionality is common among disability parking placard applications nationwide.
Disabled Veteran Parking Placard Applications: Similar to the BFS 108 form, applications for disabled veteran parking placards require verification of disability status, often with certification from the Department of Veterans Affairs or a medical professional. While the target demographic and specific qualifications might differ, the essence of the application process—providing proof of eligibility for special parking accommodations—is consistent.
Disability License Plate Application Forms: In addition to placards, many jurisdictions offer disability license plates. These applications, like the BFS 108 form, typically require a medical certification of disability. The process involves providing detailed information about the eligible vehicle and its owner, underscoring the forms' emphasis on confirming both the disability and the ownership of the vehicle for which the license plate is issued.
Wheelchair Symbol License Plate Applications: Similar again to the BFS 108, applications for license plates bearing the international symbol of access also require medical certification of a permanent or, in some cases, temporary disability that impairs mobility. The primary objective is to provide visual recognition of the right to use designated parking spaces, aligning the application's purpose closely with that of the BFS 108 form.
Free Parking for Disabled Individuals Applications: Particular segments of the BFS 108 form address eligibility for free parking, a provision not universally available. Comparable applications in other regions may have separate documents for this purpose, focusing on individuals with severe mobility impairments or those who cannot operate parking meters due to physical limitations. The selection criteria and the need for professional certification echo the BFS 108’s third section.
Organizational Disability Placard Applications: For organizations that transport individuals with disabilities, the BFS 108 includes a segment dedicated to applying for placards for organizational use. This aspect is mirrored in other jurisdictions' forms that cater to the needs of service providers, rehabilitation centers, and care homes, offering a streamlined way to obtain necessary parking permissions for vehicles used in service of individuals with disabilities.
Dos and Don'ts
When filling out the BFS 108 Michigan Disability Parking Placard Application, it’s important to follow certain guidelines to ensure a smooth and accurate process. The following is a list of things you should do, as well as things you shouldn't do, to help you successfully complete the application.
Do:
- Read all the instructions provided on the form carefully before filling it out.
- Ensure the disabled person or an authorized representative completes and signs Part 1 of the application.
- Have a licensed physician, chiropractor, optometrist, nurse practitioner, or physician’s assistant complete and sign Part 2, verifying the disability.
- Check if you qualify for free parking under Part 3, and if applicable, have it completed and signed by a medical professional.
- If you are applying on behalf of an organization, accurately fill out Part 4, providing details about the transportation services offered to persons with disabilities.
- Confirm that all the information provided on the form is accurate and true to avoid penalties.
- Attach a copy of the medical waiver if the applicant has a CDL endorsement and answered ‘yes’ to having a medical waiver.
- Ensure the medical professional includes their medical license number, which is a required field for processing the application.
- Keep a copy of the completed application for your records before submitting.
- Submit the completed form either in person at any Secretary of State branch office or mail it to the address provided on the form.
Don't:
- Leave any section of the application blank. Incomplete applications cannot be processed.
- Forget to sign and date the application in the designated areas for both the applicant (or representative) and the certifying medical professional.
- Use outdated or incorrect information, as this could delay the application process or result in denial.
- Manipulate or falsely represent the applicant's condition. Making a false statement on this application is subject to penalties.
- Attempt to fill out Part 2 or Part 3 unless you are a licensed medical professional authorized to certify the disability and eligibility for free parking, if applicable.
- Ignore the requirements for free parking eligibility. Make sure you meet the specific conditions listed under Part 3 before applying.
- Overlook the physician’s instructions to attach a copy of their out-of-state medical license if their license was not issued in Michigan.
- Mail the application without ensuring all parts are accurately completed and signed.
- Use the placard for benefits other than those it is intended for, as misuse can result in fines or imprisonment.
- Forget to promptly return the parking placard to the Secretary of State for cancellation if the organization ceases to provide specialized transportation services to disabled persons.
Misconceptions
When it comes to the BFS 108 Michigan form, otherwise known as the Disability Parking Placard Application, there are quite a few misconceptions floating around. Understanding these can save individuals a lot of confusion and ensure that those who are eligible for a placard can obtain it without unnecessary hurdles. Here are five common myths debunked:
- Only drivers can apply for a disability parking placard.
This is not true. While the form does inquire about Michigan driver's license or ID card numbers, it's important to note that non-drivers with disabilities are also eligible to apply for a placard. This ensures that anyone who meets the medical eligibility criteria can benefit from the use of disability parking, regardless of their driving status.
- The application form is for individuals only.
Actually, the BFS 108 Michigan form accommodates both individuals and organizations. Part 4 of the form is specifically designed for organizations that provide transportation services to persons with disabilities. This allows these groups to obtain parking placards for their vehicles, ensuring easier access to various locations for individuals under their care.
- Economic need is a factor in determining eligibility.
When it comes to the issuance of a disability parking placard, economic need does not play any role. Part 3 of the form, which deals with the application for free parking, makes it clear that financial considerations are not taken into account. Eligibility is solely based on the medical criteria outlined in the form.
- A medical license from another state is not acceptable.
On the contrary, if a physician licensed in another state is certifying the application, they simply need to submit a copy of their medical license alongside the BFS 108 form. This flexibility ensures that patients who are seeing out-of-state specialists can still apply for a placard.
- Only permanent conditions qualify for a disability parking placard.
The form distinguishes between permanent and temporary conditions, allowing for both to qualify for a placard. It's a common misconception that only lifelong disabilities are eligible. In reality, temporary conditions with significant mobility limitations can also make one eligible, with the placard's validity reflecting the estimated duration of the condition.
Understanding these misconceptions can help simplify the process of applying for a disability parking placard in Michigan. It's all about ensuring that those who truly need these placards can obtain them with as little hassle as possible.
Key takeaways
Filling out the BFS 108 Michigan form is a necessary step for individuals and organizations in Michigan seeking disability parking placards, which can also include an option for free parking under certain conditions. Here are key takeaways to guide you through the process:
- Part 1 requires personal information and signature: The applicant must fill in their personal details, including their name, date of birth, and contact information. They must also sign the form, authorizing the release of their medical information to the Michigan Department of State. This part is critical for verifying the applicant's identity and residency.
- Medical certification is mandatory: Part 2 of the form has to be completed by a qualified medical professional. This section is designed to establish the medical eligibility of the applicant based on their mobility challenges. The certifying professional must indicate whether the disability is permanent or temporary, and if temporary, specify the duration, up to a maximum of six months.
- Eligibility for free parking requires additional certification: If the applicant is eligible for free parking, Part 3 must also be completed by the medical professional. This section focuses on specific conditions that hinder the individual's ability to use standard parking meters and tickets. It's important to note, however, that economic need is not considered for eligibility.
- Organizations can apply for multiple placards: Part 4 allows organizations that provide transportation services for disabled persons to request parking placards. The organization must describe the services it offers and specify the number of placards needed. This provision ensures that groups catering to multiple individuals with disabilities have adequate access to designated parking.
- It’s crucial to avoid false statements: The form and accompanying regulations make it clear that providing false information, altering or selling placards, and other forms of misuse are punishable offenses. These strict measures help protect the integrity of the program and ensure that those who genuinely need these placards have access to them.
Overall, the BFS 108 form serves as a crucial tool for individuals and organizations in Michigan, facilitating accessible parking for those with mobility impairments. Careful adherence to the guidelines ensures a smooth application process and helps maintain the system’s effectiveness.
Popular PDF Templates
Is Car Insurance Required in Michigan - It also functions as a deterrent against allowing uninsured driving, with stark warnings about liability and penalties.
Death Certificate Records - Includes a provision for detailing the type of business or industry the deceased was involved in during their lifetime.
Michigan Ri 59 - Available on the Michigan State Police website, it is easily accessible for dealers needing to comply with PA 265 of 2000.